Introduction
For radiologists, the “false positive” is the enemy. It leads to unnecessary biopsies, skyrocketing healthcare costs, and immense psychological distress for patients. In breast cancer screening, the recall rate has historically hovered around 10-12% in the US. However, as we close 2025, a new generation of Deep Learning (DL) models is fundamentally changing this statistic.
It is not about replacing the radiologist; it is about creating a “super-reader.”
The Problem: Tissue Overlap
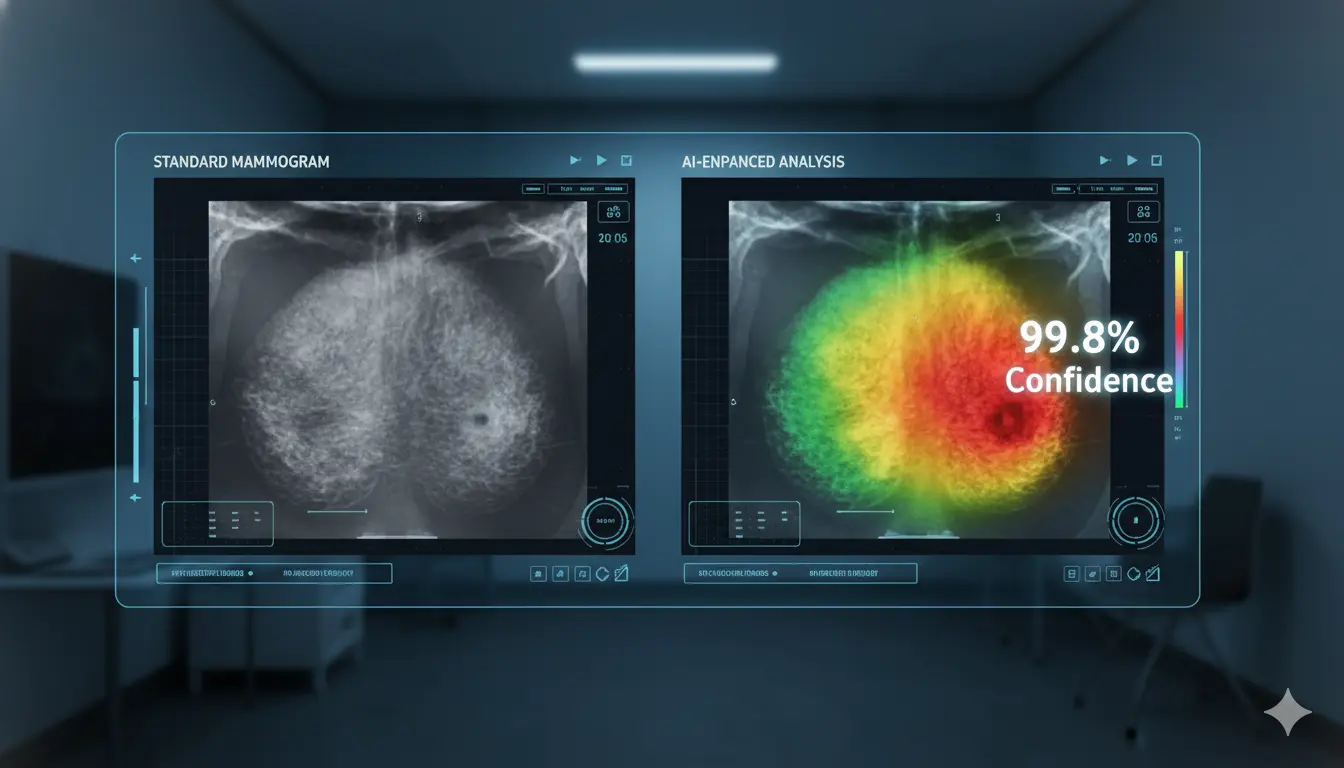
The primary challenge in 2D mammography is that breast tissue is 3D. When flattened, normal tissues can overlap, creating shadows that look like tumors (summation artifact). Conversely, dense tissue can hide actual tumors.
The AI Solution: Computer-Aided Detection (CAD) 2.0
Old CAD systems from the 2010s were notorious for marking everything, forcing doctors to ignore them. The 2025 AI models, trained on millions of biopsy-proven images, function differently.
- Pattern Recognition: Instead of just looking for bright spots, these models analyze the texture and architectural distortion of the tissue.
- The Heatmap: When a radiologist opens a scan, the AI waits. If the radiologist marks a scan as “normal,” the AI runs a background check. If it detects a high-probability lesion, it prompts the doctor: “Review region B—calcification cluster detected.”
Clinical Impact Data
A multi-center study released this month involving 50,000 screenings demonstrated the impact of this workflow:
- Reduction in Recalls: The AI-assisted group saw a 30% drop in false recalls.
- Earlier Detection:Â The AI flagged subtle micro-calcifications in dense breasts an average of 11 months earlier than standard review.
- Workflow Efficiency:Â While it seems like adding AI would slow things down, it actually sped up read times by 15% because doctors spent less time analyzing clearly benign cysts.
Implementation for Hospital Admins
For administrators, the ROI is clear. A reduction in unnecessary follow-up imaging clears schedules for patients who actually need care. The barrier to entry remains integration—hospitals must ensure their PACS (Picture Archiving and Communication System) is cloud-compatible to handle the processing load of these heavy DL models.