Introduction
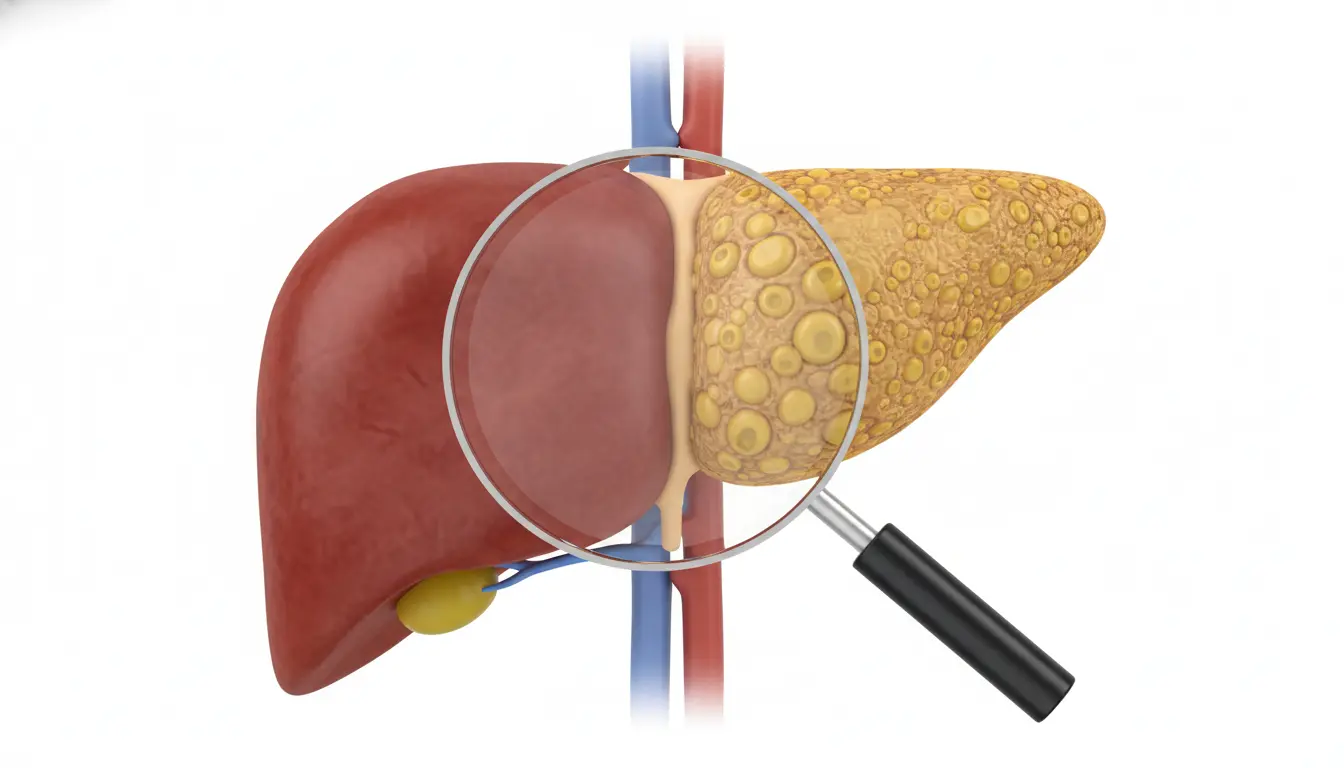
The nomenclature has changed, and so has the urgency. What we used to call Non-Alcoholic Fatty Liver Disease (NAFLD) is now MASLD (Metabolic Dysfunction-Associated Steatotic Liver Disease). It is a silent epidemic, affecting nearly 30% of the global adult population.
The danger of MASLD is its silence. Patients have no symptoms until they reach late-stage cirrhosis. For General Practitioners (GPs) in 2025, the goal is to catch the disease in the “steatohepatitis” (MASH) phase, where it is still reversible.
The Diagnostic Shift: No More Biopsies
In the past, diagnosing the severity of liver fat required a painful needle biopsy. Today, the standard of care has shifted to non-invasive algorithms.
- The FIB-4 Score:Â Every primary care visit for a diabetic or obese patient should include this calculation. It uses Age, AST, ALT, and Platelet count to estimate liver scarring.
- Vibration-Controlled Transient Elastography (FibroScan):Â If the FIB-4 score is elevated, patients are sent for this ultrasound-based test, which measures liver “stiffness” in minutes.
The Solution: Lifestyle + The New Pill
For years, “eat less and exercise” was the only advice doctors could give. It rarely worked long-term. In late 2025, we now have pharmacological weapons.
- Resmetirom:Â The first FDA-approved drug specifically for liver scarring. It targets thyroid hormone receptors in the liver to burn fat.
- GLP-1 Agonists (Semaglutide/Tirzepatide):Â Originally for diabetes, these drugs have shown remarkable ability to reduce liver fat. By helping patients lose 15-20% of their body weight, the liver automatically begins to repair itself.
Clinical Takeaway
Doctors must stop viewing fatty liver as a “benign” finding on an ultrasound. It is a metabolic warning sign. By combining aggressive weight management (via GLP-1s) with regular FIB-4 monitoring, we can prevent the progression to cirrhosis.